Pulmonary Embolism – Clinical Risk Assessment Tools
Adil Abbasi, MD, FACP
Quick Clinical Summary: How to Measure Each Scale/Tool
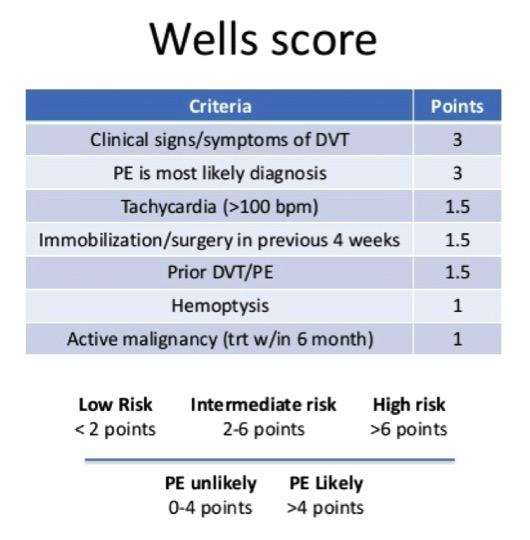
1. Wells Score (Diagnosis)
How to Measure (Step-by-Step)
Step 1: Assign points
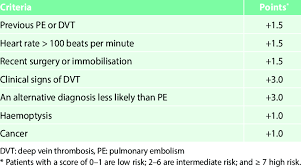
Variable | Points |
Clinical signs of DVT | +3 |
PE most likely diagnosis | +3 |
HR >100 | +1.5 |
Immobilization/surgery (4 weeks) | +1.5 |
Prior DVT/PE | +1.5 |
Hemoptysis | +1 |
Cancer | +1 |
Step 2: Add total score
Step 3: Interpret
Score | Probability |
≤4 | PE unlikely |
>4 | PE likely |
What You Do Next
Reinforcement
2. Revised Geneva Score (Diagnosis)
How to Measure
Step 1: Assign points (objective only)
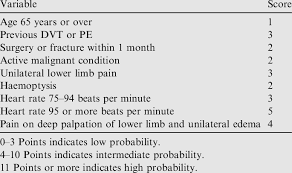
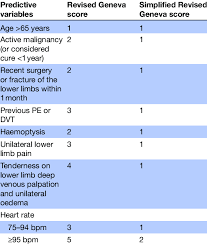
Variable | Points |
Age >65 | +1 |
Prior DVT/PE | +3 |
Surgery/fracture (1 month) | +2 |
Active cancer | +2 |
Unilateral leg pain | +3 |
Hemoptysis | +2 |
HR 75–94 | +3 |
HR ≥95 | +5 |
Pain on leg palpation | +4 |
Step 2: Add score
Step 3: Interpret
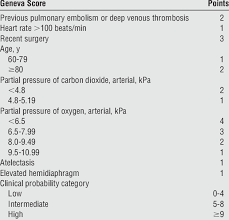
Score | Probability |
0–3 | Low |
4–10 | Intermediate |
≥11 | High |
Reinforcement
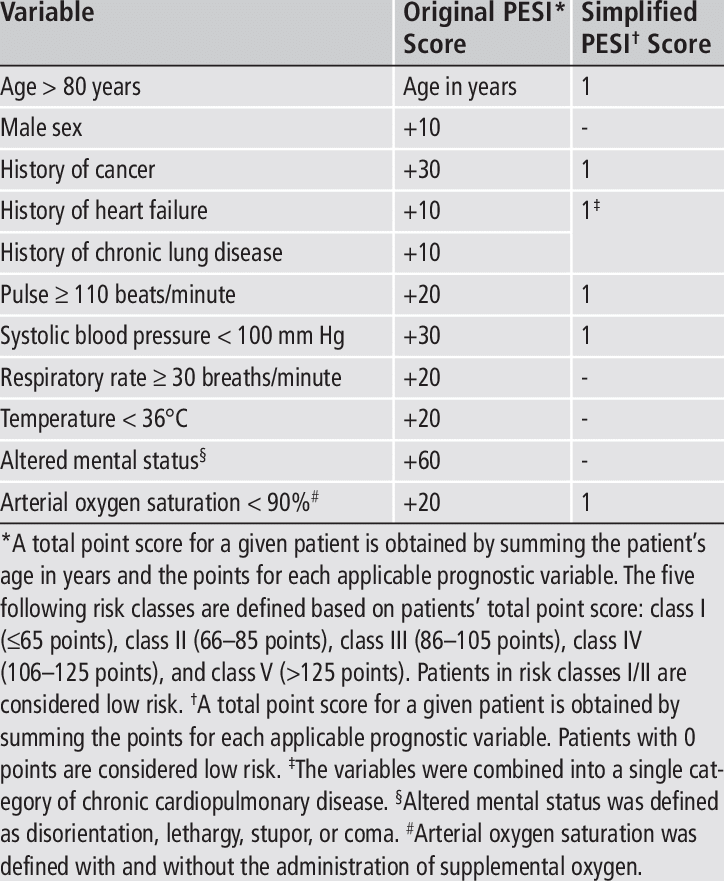
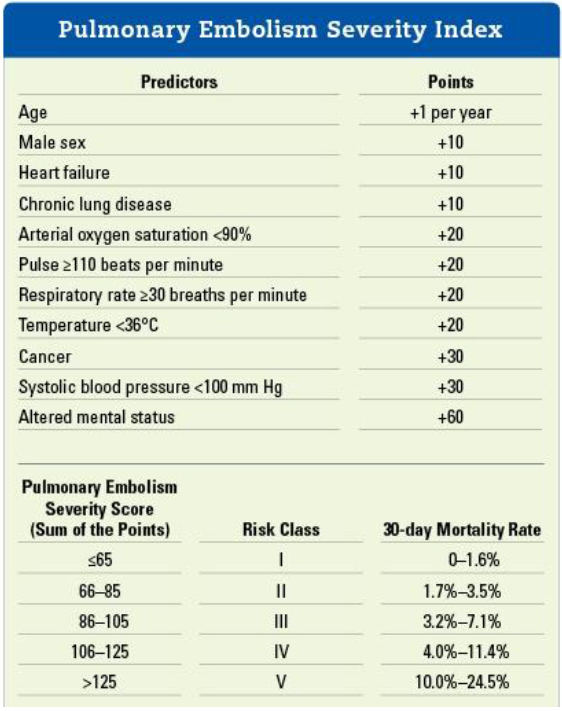
3. PESI Score (Mortality Risk)
4
How to Measure
Step 1: Start with age (baseline score = age)
Step 2: Add points
Variable | Points |
Male sex | +10 |
Cancer | +30 |
Heart failure | +10 |
Chronic lung disease | +10 |
HR ≥110 | +20 |
SBP <100 | +30 |
RR ≥30 | +20 |
Temp <36°C | +20 |
Altered mental status | +60 |
O2 sat <90% | +20 |
Step 3: Total score → classify
Class | Score | Mortality |
I | ≤65 | Very low |
II | 66–85 | Low |
III | 86–105 | Moderate |
IV | 106–125 | High |
V | >125 | Very high |
Reinforcement
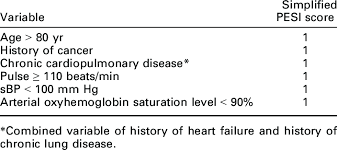
4. sPESI (Simplified PESI)
How to Measure
Step 1: Give 1 point for each:
Step 2: Total
Score | Interpretation |
0 | Low risk |
≥1 | Higher risk |
Reinforcement
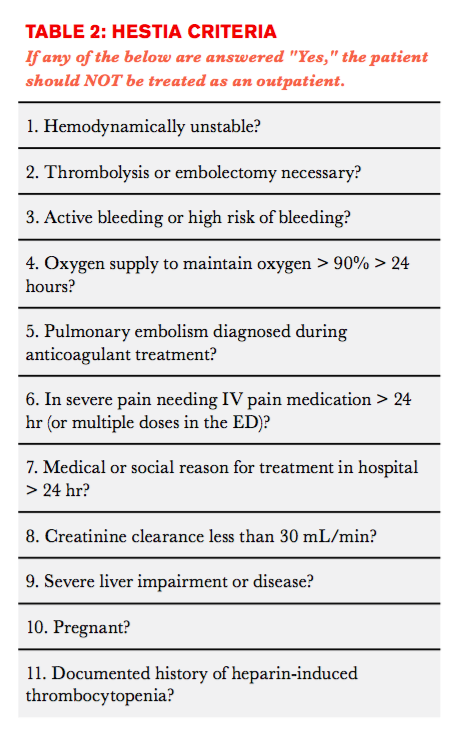
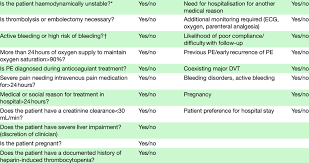
5. Hestia Criteria (Disposition)
How to Measure
Step 1: Go through checklist (YES/NO)
Key domains:
Step 2: Interpretation
👉 If ANY = YES → NOT outpatient
👉 If ALL = NO → safe for discharge
Reinforcement
Ultra-High Yield Summary Table
Tool | How to Measure | Output | Key Use |
Wells | Add weighted points (includes judgment) | Likely vs unlikely | Diagnosis |
Geneva | Add objective points | Low/intermediate/high | Diagnosis |
PESI | Age + weighted variables | Class I–V | Mortality |
sPESI | 6 variables (0 or 1) | Low vs high risk | Quick mortality |
Hestia | Yes/No checklist | Safe vs unsafe discharge | Disposition |
One-Minute Bedside Workflow
Final Reinforcement (Memory Anchor)
If you want, I can next create:
✔️ A single-page printable cheat sheet
✔️ OR case-based scenarios (like real ER cases using these scores together)
A single-page printable cheat sheet
Here is a clean, single-page printable cheat sheet designed for real bedside use (ER / inpatient / exam review). You can copy-paste into Word/PDF and print.
🫁 ACUTE PULMONARY EMBOLISM (PE) – ONE-PAGE CHEAT SHEET
1. CLINICAL FLOW (MEMORY ANCHOR)
Suspect → Diagnose → Risk → Disposition → Treat
2. DIAGNOSIS (PRETEST PROBABILITY)
WELLS SCORE
Variable | Points |
Signs of DVT | +3 |
PE most likely | +3 |
HR >100 | +1.5 |
Surgery/immobilization | +1.5 |
Prior DVT/PE | +1.5 |
Hemoptysis | +1 |
Cancer | +1 |
Interpretation:
GENEVA SCORE (OBJECTIVE)
Variable | Points |
Age >65 | +1 |
Prior DVT/PE | +3 |
Surgery/fracture | +2 |
Cancer | +2 |
Leg pain | +3 |
Hemoptysis | +2 |
HR 75–94 | +3 |
HR ≥95 | +5 |
Leg tenderness | +4 |
Interpretation:
DIAGNOSTIC ALGORITHM
3. MORTALITY RISK (AFTER DIAGNOSIS)
sPESI (FAST TOOL)
1 point each:
Score:
PESI (DETAILED)
Start = Age (base score)
Add:
Variable | Points |
Male | +10 |
Cancer | +30 |
CHF | +10 |
Lung disease | +10 |
HR ≥110 | +20 |
SBP <100 | +30 |
RR ≥30 | +20 |
Temp <36 | +20 |
AMS | +60 |
O2 sat <90% | +20 |
Classes:
4. DISPOSITION (Hestia Criteria)
YES/NO CHECKLIST
Ask:
Interpretation:
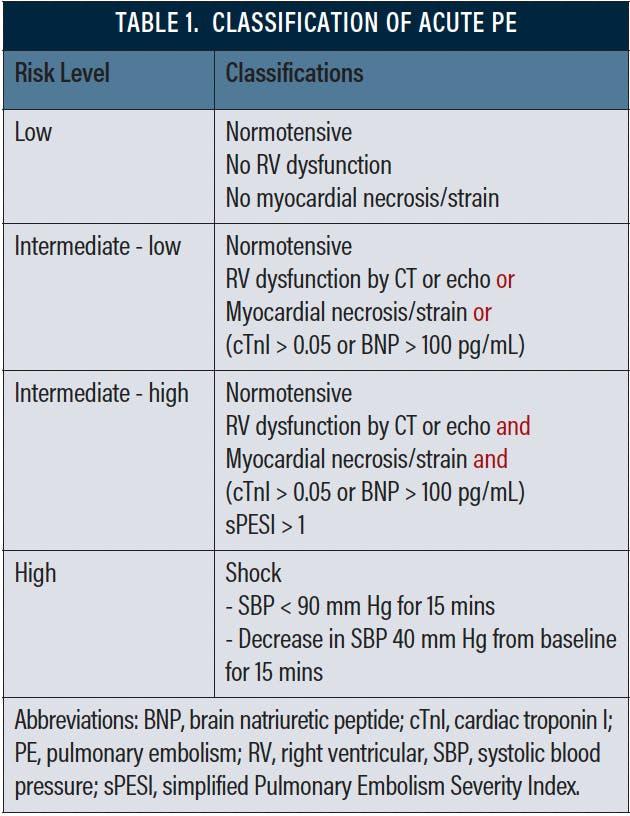
5. RISK CLASSIFICATION (A–E)
Category | Meaning | Action |
A | Asymptomatic | Outpatient |
B | Low risk | Outpatient |
C | RV strain/biomarkers | Admit |
D | Deteriorating | ICU |
E | Shock | Thrombolysis |
6. RV STRAIN (KEY PROGNOSTIC FACTOR)
CT
Echo
7. BIOMARKERS
Marker | Meaning |
D-dimer | Diagnosis only |
Troponin ↑ | RV injury |
BNP ↑ | RV strain |
8. ANTICOAGULATION
FIRST-LINE
LMWH (Enoxaparin)
UFH (CRITICAL USE ONLY)
Use if:
9. TREATMENT BY SCENARIO
Scenario | Treatment |
Stable outpatient | DOAC |
Stable inpatient | DOAC/LMWH |
Category C | Admit + anticoagulation |
Category D | ICU + UFH |
Category E | Thrombolysis |
10. REPERFUSION DECISION
11. DURATION OF ANTICOAGULATION
Scenario | Duration |
All PE | ≥3 months |
Provoked | 3 months |
Unprovoked | 3–6+ months |
Recurrent/persistent | Indefinite |
12. DISCHARGE CRITERIA
13. HIGH-YIELD PEARLS
FINAL MEMORY LINE
👉 “Wells finds it → PESI grades it → Hestia places it → RV defines it → DOAC treats it.”